
The Diagnostic Question
We have more diagnostic technology than ever. So why is it so hard to get answers?


The diagnostic question motivates many trips to the doctor. We might go to the doctor for a variety of reasons—occupational physical, school physical, advice about disease prevention—but mainly, we go because we’re ill. Illness can take many forms, of course. My tooth hurts. There’s a red bump on my leg. I’m bleeding from my belly button. I feel weird for 2 seconds every time I stand up. My muscles feel like they’re burning. And so on.
In each instance when we bring our illness to the doctor, we naturally ask the diagnostic question: “what’s wrong with me?”
What the experience of illness contains, in each of these cases, is an awareness that something is wrong; more precisely, something is wrong with my body. To the philosopher, this is interesting in the way that illness takes the body, normally a tool that is ready at hand for us to use, and makes it a burden; the ill body seems to stand like an obstacle between us and our everyday life. To the physician, on the other hand, illness is in itself a thing to be discerned. When a patient enters the clinic to ask, “what is wrong with me?” we proceed as though there is a “what” waiting to be uncovered.
For a bit over 100 years1, the training of doctors has focused primarily on listing and detecting those “whats,” chiefly for the purpose of reacting to them with some form of treatment. For much of that time, the methods of detection weren’t much more sophisticated than they had been for several centuries before. The doctor’s senses and a handful of rudimentary diagnostic tests were the extent of the available investigative methods. For example, in diabetes mellitus, diabetes refers to the voluminous flow of urine seen in diabetics, and mellitus derives from the Latin word for honey, meaning “honey-sweet.” How the disease came to be referred to thusly—“honey-sweet urine”—I will let the reader ponder.
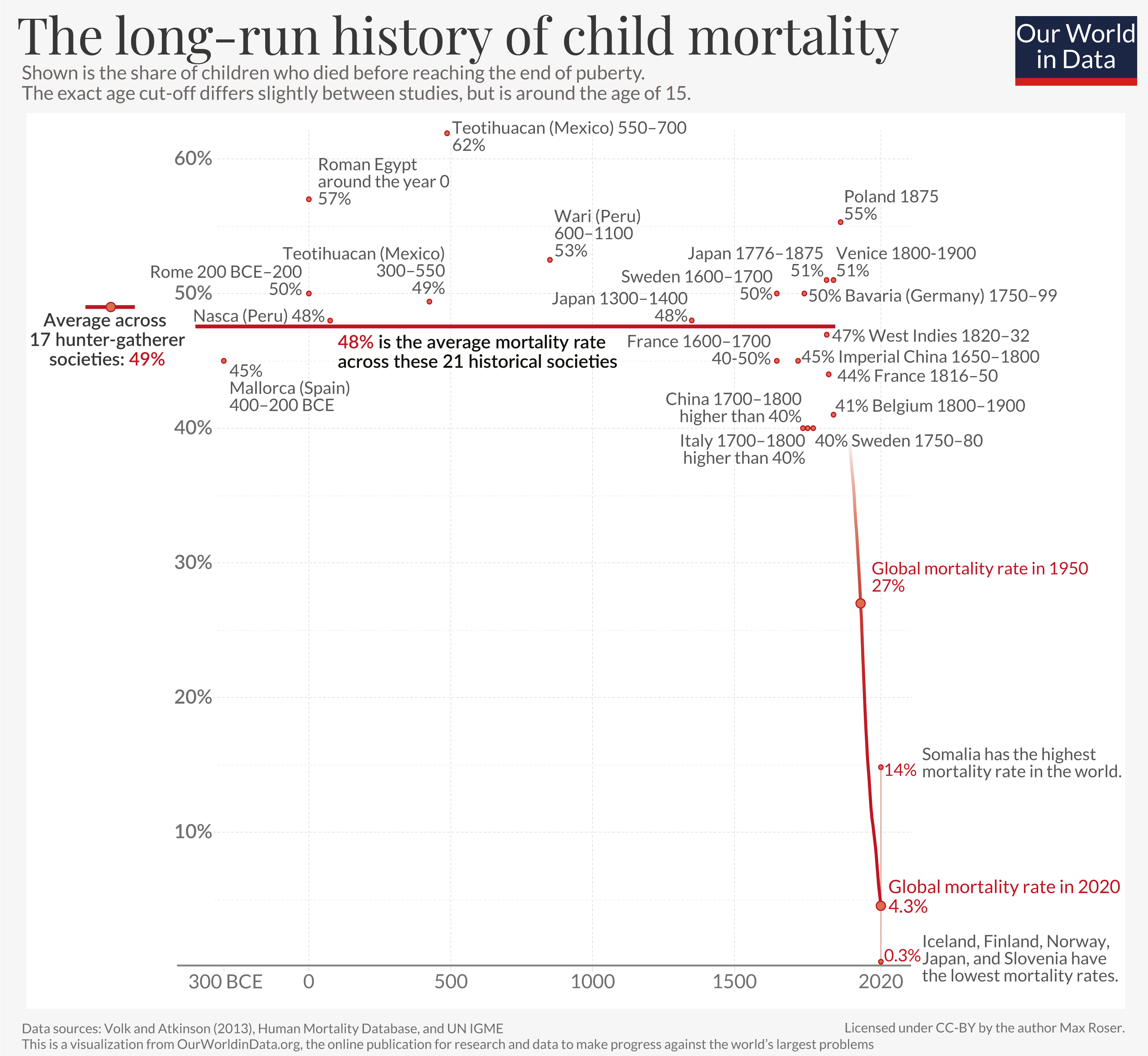
But much has changed. In the middle of the 20th century, a biomedical scientific revolution started, one whose current still sweeps us along today. Along with the development of effective treatments like antibiotics, chemotherapy for cancer, or immune-suppressing medications for autoimmune disease, tremendous progress has been made in the technologies that allow the discernment of causes of illness. Quest Diagnostics, one of the world’s largest diagnostic laboratory companies, for example offers more than 3,500 laboratory tests. Beyond mere technological triumphs, the scientific progress of biomedicine has yielded remarkable results in human wellness. To take but one example: child mortality before puberty is estimated to have declined from nearly 50% for most of human history to less than 5% globally by 2020.
In the 21st century, an individual person’s chances of dying from a tonsil infection, tuberculosis, measles, or malaria are considerably smaller than they were in the late 19th century. And yet. Despite the astounding achievements of medical science, suffering persists; as doctors we continue to confront it every day in the clinic. Although we have the benefit of sophisticated technologies like molecular laboratory analyses, high-resolution imaging, and individually targeted genetic therapies, the initial experience of illness is still mediated in much the same way it was 150 years ago: sitting in front of a doctor to ask, “what’s wrong with me?”
We doctors (as a profession, if not as individuals) have gotten demonstrably better at identifying and categorizing causes of illness. Technological progress in diagnostic technologies has aided this improvement, certainly, and not only through the sheer volume and complexity of available testing. Improvements in medical technology have also facilitated the conceptualization and delineation of entire categories of disease that would have been meaningless to a doctor in 1926, or 1826.
For example: I myself am a rheumatologist. Rheumatology as a field has a history that is interesting in its own right, and that history led to the development of a medical subspecialty that concerns itself with a broad variety of disorders and causes of illness. But for current purposes, suffice to say that rheumatology deals with many forms of autoimmune disease. Put briefly, autoimmune diseases arise when the body’s system of immunity (a word derived from the Latin term for protection, or exemption in a legal sense) stops discriminating between “self” and “not-self,” and consequently starts to apply its protective measures against microbial invasion—i.e., inflammation—to the body’s own tissues despite the absence of infection.
What’s worth pointing out here is that the concept of “autoimmunity” would have been unintelligible to a doctor in 1926. Not due to lack of intellect or education, but because the immune system itself, as a complex, constantly interacting set of cells and proteins, had not yet been described; that happened in the 1940s-60s. Moving further back, to a doctor in 1826 the concept of “immunity” itself would have been barely interpretable: the germ theory of infectious disease wasn’t fully elaborated until the 1860s-80s. All of which is to say: technological advancements in medicine don’t just expand our ability to identify causes of illness. They also expand our ability to conceive of entire categories of illness that were previously inconceivable because we lacked the empirical framework necessary to even think about them.
Let’s return to the present day.
A person walks into my rheumatology clinic and says, “what’s wrong with me?” When asked to describe the experience of their illness, they say, “for the last 3 months, my hands and feet are stiff and painful for 2 hours after I wake up, and I feel fatigued all day.” I examine their joints and find 14 joints that are swollen and tender to the touch. I order some lab tests and find high levels in the serum of rheumatoid factor and antibodies targeting citrullinated peptides. I can say confidently that this person has rheumatoid arthritis. Not only that, I can also describe in some detail precisely what is “going wrong” on a cellular and molecular basis and how that translates into the symptomatic experience of the person’s illness.
In the next exam room, I might find a person whose says, “my throat is intensely painful when I swallow, and I’ve had fevers and chills all night.” On examination I find a temperature of 102.8°F, swollen tender lymph nodes in the neck, and an angry, red throat with swollen tonsils leaking pus. We swab that pus to test for proteins or carbohydrates known to be present on the surface of streptococcus bacteria; the test is positive. I can say confidently that this person has streptococcal pharyngitis (“strep throat”). Here again, I can elaborate a detailed explanation of the invasion of body tissues by a bacteria called Streptococcus pyogenes, and the causation of the symptoms of strep throat by the inflammatory response the immune system mounts to eliminate the infection.
In both of these cases, the cause of the person’s illness is obvious to any doctor practicing in 2026. Clearly, the availability of reliable technological diagnostic methods helps to reinforce the impressions we form through history and physical examination. But what I want to draw out of both of these examples is that a doctor in 1826 would not have had the conceptual framework to even conceive of, much less name, either of these causes of illness.
From the vantage point of the early 21st century, it’s tempting to think that we have “solved” biomedicine. Equipped with our 3,500+ laboratory tests, high-resolution MRIs, and whole-genome sequencing, we can surely diagnose the cause of every illness of the people who walk through our doors... right? That question is answered (resoundingly, thunderously: NO!) if one surveys online reviews of doctors or social media communities where people share their stories of illness. As much as ever before (possibly moreso), patients feel dissatisfied with the answers—or lack thereof—offered by doctors in response to their descriptions of illness.
So, this is where I see us in clinical medicine right now. Despite the application of ever more advanced technology to discerning the causes of our patients’ illnesses, dissatisfaction with the answers doctors have to offer seems only to get worse. And of course, this is true even before we factor in the quite valid concerns about access, availability, and cost of care in the world’s healthcare systems (not least here in the U.S.). How can we make sense of this widening discrepancy? And—perhaps even more existentially—what is going to be the role of A.I. in its evolution?
In my next few posts, I plan to think more about diagnosis as a medical activity, and also about the ways that it can disappoint. I’ll also consider the possibilities of A.I. as it infiltrates clinical medicine, both for good and for ill. In the meantime, if you found this post interesting or helpful, please pass it along to someone else or provide feedback in the comments. Please also feel free to suggest any topics that you’d like to read about for future posts.
We can more or less date “modern” medical education to the publication of the Flexner Report in 1910.